Lipohypertrophy: How to Spot Insulin Injection Lumps, Treat Them, and Prevent More
Two-thirds of insulin-treated adults have lipohypertrophy in at least one site. Three habits drive most cases. Here's how to spot, treat and prevent lipo lumps.
By Daisy Lin
Medical Writer • Reviewed April 25, 2026
Lipohypertrophy is a soft, rubbery thickening of subcutaneous tissue at frequently injected sites; it does not hurt and does not look red, which is why most affected patients have not been told they have it. Two-thirds of insulin-treated adults have at least one site involved. The three habits that drive most cases are needle reuse, failure to rotate sites, and a small injection-site pool. Treatment is to stop injecting in the affected area for at least three months and let the tissue recover.
This article covers what lipohypertrophy actually is, the three habits that drive most cases, how to identify it on yourself, and what to do once you have it. It is one of the few topics in routine diabetes self-management where the patient action is straightforward and the clinical payoff is large.
What it is
Lipohypertrophy is localised hypertrophy of subcutaneous adipose tissue at frequent injection sites. To touch, it feels like a soft, rubbery cushion sitting just under the skin, distinct from the surrounding tissue, often with a slightly raised surface visible when the skin is tensioned. It does not hurt to press on. It does not look red or inflamed.
It is not the same as lipoatrophy, which is the opposite condition (localised loss of subcutaneous fat) and is largely historical with modern analogue insulins. Lipohypertrophy is the present-day issue and the one you want to avoid.
The Blanco et al. 2013 study, which screened 430 insulin-treated adults across 16 European centres, found lipohypertrophy in 64.4%, and made the point that only 32% of affected patients had been told they had it by their healthcare team. It is consistently under-detected in routine clinic visits, because it does not hurt, does not show on a glucose log directly, and the only way to find it reliably is to palpate the abdomen with the patient's clothing off.
What it does to glucose control
The Heinemann 2021 review summarises the absorption literature: insulin injected into lipohypertrophic tissue absorbs more variably, with both higher and lower peak concentrations than the same dose injected into healthy tissue. The clinical signature is unstable glucose control with no obvious cause — readings that swing for reasons unrelated to food intake or exercise.
Patients moving from injecting consistently into a lipo area to injecting into healthy tissue often need to reduce their insulin dose by 10–20% to maintain the same glucose target. This is a clinically meaningful change. It is also a reason to involve your diabetes team in the rotation switch, not to do it overnight on your own.
The three habits that drive most cases
The Blanco et al. data and the FITTER consensus converge on three risk factors that account for most cases:
1. Re-using pen needles
The single biggest preventable factor. The Blanco data showed that patients who re-used needles had roughly four times the risk of lipohypertrophy compared to single-use. The mechanism is mechanical — a re-used needle has a microscopically blunted bevel and partially stripped silicone lubrication, which causes more tissue trauma per injection. Repeated trauma at the same site leads to the chronic adipose tissue remodelling that lipohypertrophy actually is.
The cost argument that drives needle re-use is largely self-defeating: a 100-pack of 30G × 4 mm pen needles at the EU online wholesale price is around £10–14. Re-using a needle ten times to "save money" buys you a 4× higher risk of an outcome that wrecks glucose control and prompts a costlier insulin titration. We say this not because we sell pen needles (though we do) but because the arithmetic genuinely does not favour re-use. The InjectKit 30G × 5 mm pen needle 100-pack sits at the lower end of that range.
2. Failure to rotate injection sites
The second factor. Patients who consistently inject the same patch — the comfortable spot — develop lipohypertrophy specifically there. The remaining surrounding tissue stays healthy.
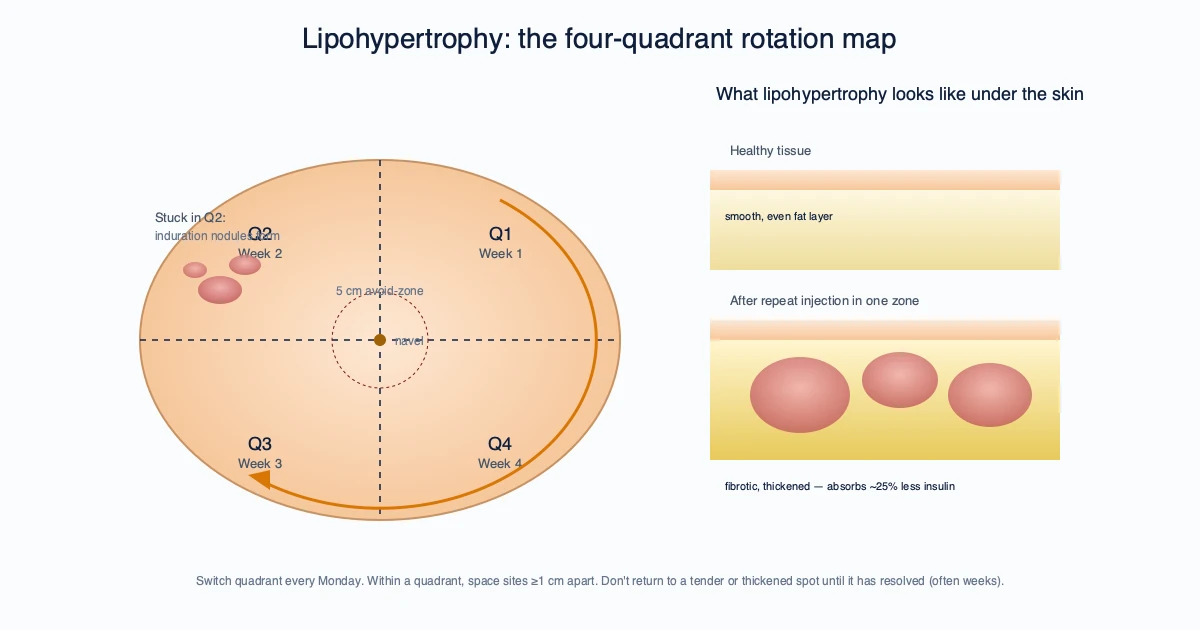
The FIT UK 5th edition recommends a clear rotation pattern, with each injection at least 1 cm from the previous, and movement between abdomen, thigh and (where appropriate) upper arm regions across the week.
3. Small injection-site pool
A patient using only a 5 cm by 5 cm patch on one side of the abdomen, even with weekly rotation within that patch, will develop lipohypertrophy faster than a patient using the full available area. The larger your injection-site pool, the more recovery time each square centimetre of tissue gets.
How to detect it on yourself
The FIT UK protocol describes a self-palpation technique that takes about two minutes:
- Stand or sit comfortably with the abdomen exposed, in good light
- With the flat of your fingers (not the fingertips), press gently on the skin in a slow circle, starting from the navel outward
- You are feeling for soft rubbery thickenings that are distinct from the surrounding tissue, usually 1–4 cm across, sometimes larger
- Compare side-to-side: a lump on the left side that is not present in the same position on the right is suggestive
- Repeat on each thigh and on the back of each upper arm if you inject there
If you find a suspect area, mark it with a non-permanent marker so you can see the boundary. Take a photo for your own records.
What to do once you have it
The published management is straightforward:
- Stop injecting in the affected area for at least three months, longer if the area is large
- Rotate to fresh injection sites — ideally a different region (move from abdomen to thigh, or from one quadrant to another)
- Talk to your diabetes team about adjusting your insulin dose. The shift to healthy tissue can change effective absorption; under-dosing in lipo tissue means you may have been dosing higher than needed, and switching to healthy tissue can produce hypoglycaemia at the same prescription
- Re-palpate at three months. The Blanco follow-up data shows most lipohypertrophic tissue resolves over 4 to 6 months without active treatment, given the injections stop
- Resume injection in the affected area only after it has resolved, and resume with a strict rotation pattern
There is no evidence to support active treatment of lipohypertrophy with massage, warm compresses, ultrasound, or any topical product. The FIT UK and FITTER documents make this point explicitly. Cessation of injection in the area, plus time, is the only treatment with published evidence.
What we recommend
For prevention:
- One injection, one needle. This is the most-effective habit. Pen needles cost pennies per injection at the EU wholesale price; the calculus does not favour re-use.
- Rotate, properly. Print a simple body diagram, mark each injection site with the date, never inject within 1 cm of the previous site within the same week.
- Use a 4 mm or 5 mm needle, not longer. Shorter needles cause less tissue trauma per injection and are sufficient for subcutaneous delivery in any adult body habitus.
- Self-palpate every three months. Two minutes with the abdomen exposed in good light catches lipohypertrophy at the early, easily reversible stage.
For detection: if your glucose control is harder to manage than the prescription should support, palpate before adjusting dose. The cause may be in the tissue, not the dial.
For treatment: stop, rotate, ask your diabetes team about dose adjustment, wait three months. Anything else is unsupported.
FAQ
Does lipohypertrophy hurt? No. It is painless to touch and to inject through, which is why it is so commonly under-detected.
How do I tell lipohypertrophy from a normal post-injection lump? A normal post-injection lump is small, slightly tender, and resolves within a couple of days. Lipohypertrophy is firm, rubbery, painless, and persists for weeks or months.
Can lipohypertrophy resolve on its own? Yes — given the area is rested. Most affected tissue resolves over 4 to 6 months without active treatment, provided injections stop.
Should I massage the lump? No. There is no evidence supporting massage, warm compresses or any topical treatment. FIT UK is explicit on this.
Does this affect GLP-1 injections too? Yes — though it is rarer at weekly dosing than at daily insulin dosing. Same prevention rules apply: rotate, do not reuse needles, do not inject through damaged tissue.
For single-use 30G × 5 mm pen needles in 100-packs, browse the 30G product range or pick up our own-label 100-pack. The cost-per-injection is well below high-street pharmacy pricing, which is the simplest path to making single-use the default.
Sources
- Blanco M, Hernández MT, Strauss KW, Amaya M. Lipohypertrophy in Insulin-Treated Diabetes. Diabetes Metab. 2013;39(5):445–453 — doi.org
- Frid AH et al. New Insulin Delivery Recommendations (FITTER). Mayo Clin Proc. 2016;91(9):1231–1255 — doi.org
- Forum for Injection Technique UK Recommendations, 5th Edition — fit4diabetes.com
- Heinemann L. Lipohypertrophy: prevalence, clinical consequences, and treatment. PMC review, 2021 — pmc.ncbi.nlm.nih.gov
- NICE NG17, Type 1 diabetes in adults — nice.org.uk
- BNF, Insulin treatment in adults with type 2 diabetes — bnf.nice.org.uk
This article is for general information only and is not medical advice. Always consult your prescriber or diabetes specialist nurse for guidance specific to your situation.
Frequently asked questions
Does lipohypertrophy hurt? +
No. It is painless to touch and to inject through, which is why it is so commonly under-detected.
How do I tell lipohypertrophy from a normal post-injection lump? +
A normal post-injection lump is small, slightly tender, and resolves within a couple of days. Lipohypertrophy is firm, rubbery, painless, and persists for weeks or months.
Can lipohypertrophy resolve on its own? +
Yes — given the area is rested. Most affected tissue resolves over 4 to 6 months without active treatment, provided injections stop.
Should I massage the lump? +
No. There is no evidence supporting massage, warm compresses or any topical treatment. FIT UK is explicit on this.
Does this affect GLP-1 injections too? +
Yes — though it is rarer at weekly dosing than at daily insulin dosing. Same prevention rules apply: rotate, do not reuse needles, do not inject through damaged tissue.
For single-use 30G × 5 mm pen needles in 100-packs, browse the 30G product range or pick up our own-label 100-pack. The cost-per-injection is well below high-street pharmacy pricing, which is the simplest path to making single-use the default.
Related reading
Insulin Storage and Travel: Fridge, Flights, Heat and the 28-Day Rule
What the EMA SmPCs actually specify for in-use insulin storage, what UK and EU airlines allow in cabin baggage, and what the 28-day rule does and doesn't mean.
Diabetes in Cats: Which Insulin Syringe and How to Dose Correctly
Diabetes in cats — choosing the right U-40 insulin syringe, drawing the dose cleanly, sterile technique and safe disposal. A complete UK practical guide.
U-100 vs U-40 Insulin Syringes: Why Pets Need a Different Scale
U-40 vs U-100 insulin syringes explained — why veterinary insulin uses a different scale, why mixing them up is dangerous, and how to pick the right one.
Get your supplies
CE-marked syringes, alcohol prep pads, and bacteriostatic water. Shipped from Spain across the EU and UK.